Key Takeaways
- Seborrheic dermatitis affects 1-3% of the general population and up to 50% of adults experience some form of it on the scalp (Journal of Clinical and Investigative Dermatology, 2015), making it one of the most widespread inflammatory scalp conditions linked to hair fall.
- The Malassezia fungus, present on over 90% of human scalps, is the primary biological trigger. It feeds on sebum and releases oleic acid, which provokes chronic inflammation that pushes hair follicles into premature shedding (telogen effluvium).
- Hair loss from seborrheic dermatitis is reversible in 85-90% of cases when the underlying inflammation is controlled within 8-12 weeks using medicated shampoos and targeted treatment.
- If hair does not regrow after seborrheic dermatitis is resolved, an overlapping condition such as androgenetic alopecia may be the true cause, affecting 50% of men by age 50 (American Hair Loss Association).
- Advanced therapies like PRP treatment and hair restoration can address permanent follicle damage that topical treatment alone cannot reverse.
Introduction
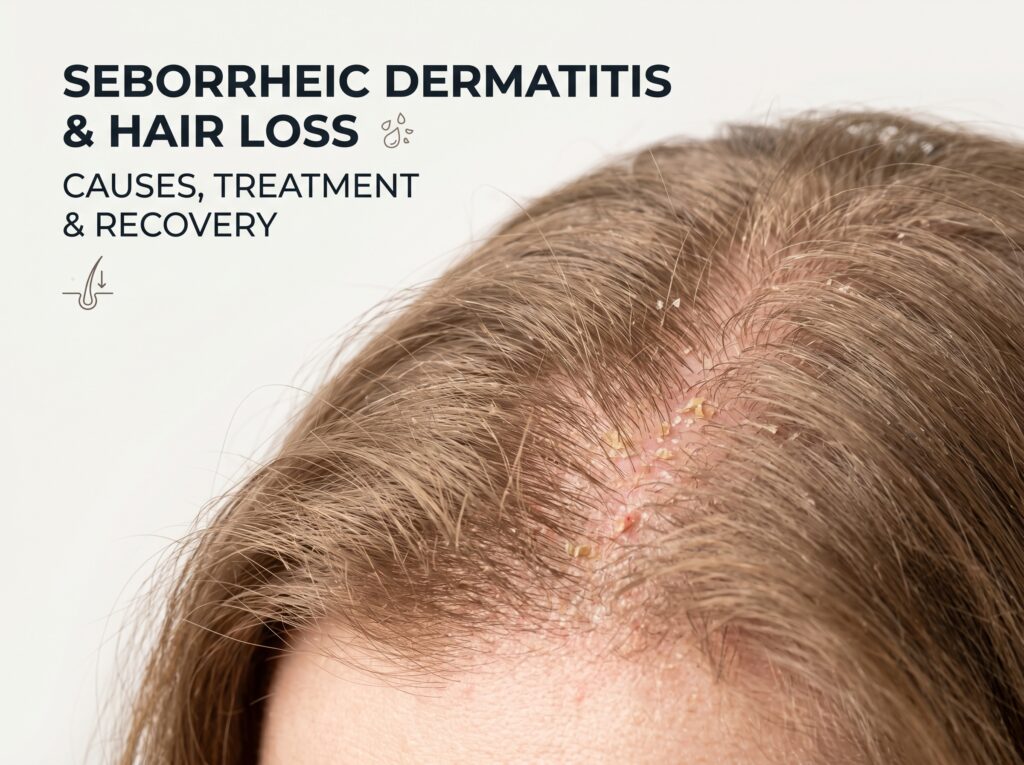
Seborrheic dermatitis is a chronic inflammatory skin condition characterised by red, greasy, scaly patches on the scalp and other sebum-rich areas of the body. It is caused primarily by an overgrowth of the Malassezia yeast, an immune-mediated inflammatory response, and excess sebum production. When it affects the scalp, it frequently leads to hair thinning and increased hair fall, a concern that brings thousands of patients to dermatology clinics each year.
If you have been dealing with persistent scalp flaking, redness, and itching alongside noticeable hair loss, you are not alone. Seborrheic dermatitis scalp involvement is one of the most under-diagnosed contributors to hair fall. Many people mistake it for simple dandruff and delay proper treatment, allowing inflammation to weaken follicles over months or years.
Dr. Abhishek Pilani, MBBS MD Dermatology (Gold Medalist, Pramukhswami Medical College), ISHRS Member and DHA Licensed dermatologist, explains: “Across 20,000+ procedures at Assure Clinic, I have observed that a significant percentage of patients presenting with diffuse hair thinning have undiagnosed or under-treated seborrheic dermatitis as a contributing factor. Once we resolve the scalp inflammation, many of these patients see meaningful hair regrowth without any surgical intervention.”
Take the Free 2-Minute Hair Loss Assessment
Answer 5 quick questions and get your personalized Norwood grade plus treatment recommendations from our doctors.
Start Free Assessment →This comprehensive guide covers the science behind seborrheic dermatitis and hair loss, the treatments that work, the shampoos dermatologists recommend, and when you should consult a specialist.
What Is Seborrheic Dermatitis?
Seborrheic dermatitis is a common, chronic, relapsing inflammatory condition that primarily affects areas of the body with a high density of sebaceous (oil-producing) glands. On the scalp, it manifests as:
- Yellowish or white greasy scales that adhere to the scalp and hair shafts
- Red, inflamed patches (erythema) beneath the scales
- Persistent itching (pruritus) that ranges from mild to severe
- Burning or stinging sensations in affected areas
The condition was first described in medical literature in the early 19th century, and today the World Health Organization recognises it as one of the most prevalent dermatological conditions globally. It can affect infants (cradle cap), adolescents, and adults, with peak prevalence in three age groups: infants under 3 months, adults between 30-60 years, and immunocompromised individuals.
How Common Is Seborrheic Dermatitis?
According to a systematic review published in the Journal of the European Academy of Dermatology and Venereology (JEADV, 2019):
- 1-3% of the general population has clinically diagnosed seborrheic dermatitis
- Up to 50% of adults experience subclinical forms (dandruff being the mildest expression)
- Males are affected more frequently than females, likely due to androgen-driven sebum production
- HIV-positive patients have a prevalence of 30-83%, indicating an immune component
Seborrheic dermatitis is not the same as simple dandruff, though they exist on a spectrum. Dandruff is the mildest form of seborrheic dermatitis limited to flaking without significant inflammation or redness.
How Seborrheic Dermatitis Causes Hair Loss
The relationship between seborrheic dermatitis and hair loss is driven by a specific biological cascade. Understanding this mechanism is essential for choosing the right treatment approach.
The Inflammation-Follicle Damage Cycle
-
Malassezia overgrowth: The Malassezia yeast (particularly M. globosa and M. restricta) feeds on triglycerides in scalp sebum, breaking them down into unsaturated fatty acids, particularly oleic acid.
-
Immune activation: Oleic acid penetrates the stratum corneum (outer skin layer) and triggers an inflammatory immune response. The body releases pro-inflammatory cytokines including IL-1, IL-6, IL-8, and TNF-alpha at the follicular level.
-
Disrupted hair cycle: Chronic inflammation around the hair follicle (perifollicular inflammation) pushes hairs prematurely from the anagen (growth) phase into the catagen (regression) and telogen (shedding) phases. This condition, known as telogen effluvium, results in diffuse hair thinning.
-
Follicular miniaturisation: Prolonged inflammation can cause follicle miniaturisation, where each successive hair cycle produces a thinner, shorter, less pigmented hair. A study in the International Journal of Trichology (2019) found that chronic seborrheic dermatitis patients showed measurable decreases in hair shaft diameter after 6+ months of untreated disease.
-
Physical damage from scratching: The intense itch drives scratching, which mechanically loosens weakened hairs and can cause traction damage to follicles. Research published in the British Journal of Dermatology (2018) documented that scratching increased daily hair fall by up to 30% in seborrheic dermatitis patients.
Is Hair Loss from Seborrheic Dermatitis Permanent?
In most cases, no. Hair loss caused by seborrheic dermatitis is reversible once the inflammation is brought under control. The follicles are not destroyed; they are suppressed. When the inflammatory environment resolves, follicles typically resume normal cycling within 3-6 months.
However, there are exceptions:
- Prolonged untreated disease (years) can lead to perifollicular fibrosis (scarring around follicles), causing permanent hair loss in affected areas
- Concurrent androgenetic alopecia may be unmasked or accelerated by seborrheic dermatitis. The hair fall reasons page explains how multiple hair loss causes frequently overlap
- Secondary bacterial infections from open scratch wounds can permanently damage follicles
Seborrheic Dermatitis vs Dandruff vs Psoriasis vs Contact Dermatitis
One of the most common diagnostic challenges is distinguishing seborrheic dermatitis from conditions that look similar. This comparison table helps clarify the differences.
| Feature | Seborrheic Dermatitis | Dandruff | Scalp Psoriasis | Contact Dermatitis |
|---|---|---|---|---|
| Appearance | Greasy, yellowish scales on red base | White or grey dry flakes | Thick, silvery-white plaques | Red, weeping, blistered patches |
| Location | Scalp, eyebrows, nasolabial folds, ears | Scalp only | Scalp, elbows, knees, lower back | Area of contact with irritant |
| Itching severity | Moderate to severe | Mild to moderate | Moderate to severe (can crack and bleed) | Intense burning and itching |
| Cause | Malassezia yeast + immune response | Mild Malassezia overgrowth | Autoimmune (T-cell mediated) | Allergic reaction to product/chemical |
| Scale type | Greasy, yellowish, soft | Dry, white, powdery | Thick, adherent, silvery | Variable, often weeping |
| Hair loss risk | Moderate to high if untreated | Low | Moderate (from scratching and plaque) | Low to moderate (temporary) |
| Chronic/recurring | Yes, lifelong with flares | Often seasonal | Yes, lifelong with flares | Resolves when trigger removed |
| Responds to antifungals | Yes (primary treatment) | Yes | No | No |
| Age of onset | 30-60 years typically | Any age | Any age (often 15-35) | Any age |
Important distinction: If your scalp condition does not respond to antifungal shampoos within 4 weeks, it may not be seborrheic dermatitis. Scalp psoriasis and alopecia areata are commonly misdiagnosed as seborrheic dermatitis, and each requires a fundamentally different treatment approach.
Causes and Risk Factors of Seborrheic Dermatitis
Seborrheic dermatitis is not caused by poor hygiene. It results from a complex interaction between three factors:
1. Malassezia Fungus Overgrowth
The Malassezia yeast is a normal part of scalp flora, present on over 90% of humans (Indian Journal of Dermatology, 2015). In seborrheic dermatitis, the issue is not simply the presence of the yeast but the body’s abnormal inflammatory reaction to its metabolic byproducts, particularly oleic acid.
2. Excess Sebum Production
Sebaceous glands in affected individuals tend to produce more sebum than normal. This excess oil provides the lipid-rich environment that Malassezia thrives in. The condition is most common in areas with the highest sebaceous gland density: scalp, face (especially nasolabial folds), and upper chest.
3. Immune Dysregulation
The disproportionately high prevalence in immunocompromised patients (30-83% in HIV patients) demonstrates that immune function plays a critical role. The immune system in SD patients overreacts to normal levels of Malassezia, triggering an inflammatory cascade that a healthy immune system would manage without visible symptoms.
Additional Risk Factors
- Stress: Psychological stress increases cortisol production, which stimulates sebaceous glands and suppresses immune function. A study in the Archives of Dermatological Research (2017) found that SD flares correlated significantly with self-reported stress levels.
- Hormonal changes: Androgens drive sebum production, explaining the higher prevalence in males and flares during puberty.
- Neurological conditions: Parkinson’s disease and stroke patients show 3-5x higher SD prevalence due to increased sebum from autonomic dysfunction.
- Weather: Cold, dry climates and low humidity worsen SD by disrupting the skin barrier.
- Nutritional deficiencies: Zinc, B-vitamins (especially B6 and biotin), and essential fatty acid deficiencies are associated with more severe SD. The essential nutrients for hair health guide covers which nutrients directly support scalp health.
- Certain medications: Lithium, buspirone, haloperidol, and some immunosuppressants can trigger or worsen SD.
Symptoms and Diagnosis
Recognising Seborrheic Dermatitis on the Scalp
The clinical presentation of seborrheic dermatitis on the scalp typically includes:
- Flaking: Greasy, yellowish or whitish scales that adhere to the scalp and hair
- Redness (erythema): Pink to red patches beneath the scales, especially along the hairline and behind the ears
- Itching (pruritus): Persistent, often worsening at night or during stress
- Burning or tenderness: Especially in acute flares
- Greasy scalp: Oily texture even shortly after washing
- Hair thinning: Diffuse thinning, particularly in areas of heaviest scale and inflammation
- Extension beyond scalp: May spread to eyebrows, eyelids (blepharitis), nasolabial folds, and ears
How Is Seborrheic Dermatitis Diagnosed?
Diagnosis is primarily clinical, meaning a qualified dermatologist can diagnose it based on visual examination and history. In some cases, additional tests include:
- Dermoscopy (trichoscopy): Magnified scalp examination revealing perifollicular scaling, arborising blood vessels, and featureless areas
- Skin biopsy: Rarely needed, reserved for atypical presentations. Shows spongiosis, neutrophilic infiltration, and parakeratosis
- Fungal culture: To rule out tinea capitis (scalp ringworm), which mimics SD
- KOH mount: Direct microscopy to identify fungal elements
If you are experiencing persistent scalp flaking and hair loss, the hair fall control page explains how Assure Clinic’s qualified doctors approach comprehensive scalp evaluation using dermoscopy and trichoscopic analysis.
Treatment Options for Seborrheic Dermatitis
Medical Treatments
Treatment follows a stepwise approach based on severity.
First-Line: Antifungal Therapy
Antifungals target the Malassezia yeast directly and are the cornerstone of SD treatment.
- Ketoconazole 2% shampoo: The gold standard. A Cochrane review (2015) confirmed ketoconazole shampoo is significantly more effective than placebo for SD. Use 2-3 times per week for 4 weeks, then once weekly for maintenance.
- Ciclopirox 1% shampoo: An alternative antifungal with anti-inflammatory properties. Effective for patients who do not respond to ketoconazole.
- Selenium sulfide 2.5%: Reduces Malassezia populations and normalises epidermal turnover.
Second-Line: Anti-Inflammatory Agents
When antifungals alone are insufficient:
- Topical corticosteroids (low to mid potency): Fluocinolone acetonide 0.01% oil or betamethasone valerate 0.1% lotion. Used for short courses (2-4 weeks) to manage acute flares. Long-term steroid use is avoided due to skin atrophy risk.
- Topical calcineurin inhibitors: Tacrolimus 0.1% ointment or pimecrolimus 1% cream. Steroid-sparing alternatives for long-term maintenance, particularly on the face.
- Zinc pyrithione: Anti-inflammatory and antifungal. Available in shampoo (1-2%) and leave-on formulations.
Third-Line: Systemic Therapy (Severe Cases)
Reserved for widespread or treatment-resistant SD:
- Oral itraconazole: 200mg/day for 1 week per month (pulse therapy)
- Oral fluconazole: 200-300mg weekly for 2-4 weeks
- Low-dose isotretinoin: Reduces sebum production in severe, recalcitrant cases
Adjunctive Hair Loss Treatments
When seborrheic dermatitis has caused significant hair thinning, addressing the inflammation alone may not be sufficient to restore full density. Evidence-based adjunctive treatments include:
- PRP (Platelet-Rich Plasma) therapy: Concentrated growth factors injected into the scalp stimulate dormant follicles and improve hair density. A meta-analysis in Dermatologic Surgery (2019) showed PRP increased hair count by 30-40% in treated areas.
- GFC (Growth Factor Concentrate) therapy: A next-generation platelet concentrate with higher growth factor concentrations than traditional PRP.
- QR678 growth factor therapy: A combination of growth factors and peptides applied topically to stimulate follicle activity.
- Minoxidil 5%: FDA-approved topical treatment that prolongs the anagen phase and improves blood flow to follicles. See our guide on DHT blockers and hair loss for how hormonal and topical treatments work together.
Dr. Abhishek Pilani, MBBS MD Dermatology (Gold Medalist) and ISHRS Member, notes: “The mistake many patients make is treating the seborrheic dermatitis and then waiting indefinitely for hair to return. If the follicles have been suppressed for more than 12 months, they often need active stimulation through PRP or growth factor therapy to resume normal cycling. We take a phased approach: control the inflammation first, then stimulate regrowth.”
Home Remedies and Natural Approaches
While medical treatment is the foundation of SD management, certain home remedies can support treatment and reduce flare frequency:
- Tea tree oil (5% concentration): A study in the Journal of the American Academy of Dermatology (2002) found 5% tea tree oil shampoo significantly reduced SD severity compared to placebo. Its antifungal (terpinen-4-ol) and anti-inflammatory properties make it a useful adjunct.
- Apple cider vinegar rinse (1:3 dilution): The acidity (pH 2-3) helps restore normal scalp pH (4.5-5.5), creating an environment less favourable for Malassezia growth. Use once weekly after shampooing.
- Aloe vera gel: Anti-inflammatory and moisturising. Apply to affected areas for 20-30 minutes before washing.
- Coconut oil: Contains lauric acid with antifungal properties. However, it is comedogenic and may worsen SD in some patients. Patch-test first.
- Omega-3 fatty acid supplementation: Anti-inflammatory effects may reduce flare severity when taken consistently (2-3g EPA+DHA daily).
Caution: Home remedies should complement, not replace, medical treatment. If your symptoms persist beyond 4 weeks of consistent home treatment, consult a dermatologist.
Seborrheic Dermatitis Shampoo Guide
Choosing the right shampoo is often the single most impactful treatment decision for scalp seborrheic dermatitis. The following table compares the major active ingredients available.
| Active Ingredient | Concentration | Mechanism of Action | Best For | Usage Frequency | Evidence Level |
|---|---|---|---|---|---|
| Ketoconazole | 1-2% | Antifungal (inhibits ergosterol synthesis) | Moderate-to-severe SD, proven first-line | 2-3x/week (treatment), 1x/week (maintenance) | Strong (Cochrane-reviewed) |
| Zinc pyrithione | 1-2% | Antifungal + anti-inflammatory + anti-sebum | Mild-to-moderate SD, maintenance therapy | Daily to 3x/week | Strong |
| Selenium sulfide | 1-2.5% | Antifungal + reduces epidermal turnover | Moderate SD, heavy flaking | 2x/week | Moderate |
| Ciclopirox olamine | 1-1.5% | Broad-spectrum antifungal + anti-inflammatory | Ketoconazole non-responders | 2-3x/week | Strong |
| Coal tar | 0.5-5% | Anti-inflammatory + anti-proliferative | Thick scale, psoriasis overlap | 1-2x/week | Moderate |
| Salicylic acid | 2-3% | Keratolytic (removes scale buildup) | Heavy crusting, as prep before antifungal | 1-2x/week | Moderate |
| Piroctone olamine | 0.5-1% | Antifungal (newer generation) | Mild SD, cosmetically-conscious patients | Daily use safe | Moderate |
| Tea tree oil | 5% | Natural antifungal + anti-inflammatory | Patients preferring natural options | 3-5x/week | Moderate |
Shampoo Application Tips
For maximum effectiveness:
- Wet hair thoroughly before applying shampoo
- Massage into scalp for at least 3-5 minutes before rinsing. Most people rinse too quickly for the active ingredient to work.
- Leave on for 5 minutes on the first application, then lather and rinse a second time
- Rotate between two active ingredients every 2-3 months to prevent Malassezia resistance
- Follow with a gentle conditioner on the lengths only (avoid scalp) to prevent dryness
When Hair Loss from Seborrheic Dermatitis Becomes Permanent
While most SD-related hair loss is reversible, certain warning signs indicate that permanent damage may have occurred:
Signs of Irreversible Hair Loss
- Hair does not regrow within 6 months of successfully treating the seborrheic dermatitis
- Visible scalp (reduced density) in areas that were previously covered
- Smooth, shiny scalp patches where follicles have been replaced by scar tissue
- Progressive Norwood or Ludwig pattern suggesting concurrent androgenetic alopecia
- Trichoscopy reveals follicular dropout: No vellus or miniaturised hairs in thinning areas
The Overlap Problem: SD + Androgenetic Alopecia
One of the most critical clinical scenarios is when seborrheic dermatitis and androgenetic alopecia (AGA) coexist. Research published in the Indian Journal of Dermatology (2020) found that 42% of male patients presenting with SD-related hair complaints also had evidence of underlying AGA.
In these cases:
- Treating the SD resolves the flaking and inflammation but does not stop the genetic hair loss
- The patient assumes “nothing is working” when in reality two separate conditions need two separate treatments
- A comprehensive evaluation including trichoscopy, pull test, and family history assessment is essential
Use the Baldness Calculator to assess your risk of pattern hair loss independent of seborrheic dermatitis.
When to See a Specialist
Consult a dermatologist or hair loss specialist if:
- Over-the-counter antifungal shampoos have not improved your condition after 4 weeks of consistent use
- Hair loss is worsening despite improvement in flaking and itching
- You notice patchy bald spots (may indicate alopecia areata rather than SD)
- The condition spreads beyond the scalp to the face, chest, or other areas
- You experience pain, oozing, or crusting suggesting secondary bacterial infection
- You have a family history of baldness and want to rule out androgenetic alopecia
At Assure Clinic, our 60+ qualified doctors across 13 locations in India and Dubai provide comprehensive scalp evaluation using advanced dermoscopy and trichoscopic analysis. The initial consultation includes a detailed scalp examination, hair pull test, and personalised treatment plan that addresses both the inflammatory condition and any concurrent hair loss.
Book a consultation: Call +91 95861 22444 or WhatsApp the same number.
Expert Insight from Dr. Abhishek Pilani
“Seborrheic dermatitis is one of the most treatable causes of hair loss, yet I see patients who have suffered for years simply because they were told it was ‘just dandruff.’ The distinction matters. Dandruff responds to basic zinc pyrithione shampoo. Seborrheic dermatitis requires targeted antifungal therapy, often combined with anti-inflammatory agents and, in cases of established hair thinning, regenerative treatments like PRP. At Assure Clinic, our approach is phased: we first eliminate the inflammation, then assess whether follicles are recovering on their own or need active stimulation. With 20,000+ cases behind us, we have seen that this phased strategy achieves the best outcomes for patients dealing with both scalp disease and hair loss.”
— Dr. Abhishek Pilani, MBBS MD Dermatology (Gold Medalist, Pramukhswami Medical College), ISHRS Member, DHA Licensed, Founder of Assure Clinic
Patients with persistent seborrheic dermatitis often benefit from combined dermatological treatment plus restoration if hair density has dropped. Our Mumbai dermatology and hair transplant clinic offers both pathways in a single consultation — no need to coordinate across multiple specialists.
10 Frequently Asked Questions
Can seborrheic dermatitis cause permanent hair loss?
In most cases, no. Seborrheic dermatitis causes reversible hair loss through inflammation-driven telogen effluvium. Once the scalp inflammation is controlled with appropriate antifungal and anti-inflammatory treatment, hair typically begins regrowing within 3-6 months. However, prolonged untreated seborrheic dermatitis (lasting years) can lead to perifollicular fibrosis (scarring around follicles), which may cause permanent hair loss in affected areas. If you have had SD for more than 12 months without treatment, consult a specialist promptly.
What is the difference between seborrheic dermatitis and dandruff?
Dandruff is the mildest form of seborrheic dermatitis, limited to dry white flaking without significant inflammation or redness. Seborrheic dermatitis is the clinical-grade condition involving greasy yellowish scales, underlying erythema (redness), moderate-to-severe itching, and potential extension to the face and other sebum-rich areas. Both involve Malassezia yeast, but SD involves a more pronounced inflammatory immune response.
What is the best shampoo for seborrheic dermatitis?
Ketoconazole 2% shampoo is the gold standard, supported by Cochrane-level evidence. Use it 2-3 times per week during active flares and once weekly for maintenance. For mild cases, zinc pyrithione 1-2% shampoo used daily is effective. If ketoconazole does not work within 4 weeks, ciclopirox 1% is a strong alternative. Rotating between two different active ingredients every 2-3 months helps prevent Malassezia resistance.
Does seborrheic dermatitis go away on its own?
Seborrheic dermatitis is a chronic condition that follows a relapsing-remitting pattern. Flares may resolve spontaneously but will typically return, especially during stress, seasonal changes, or immune suppression. While it cannot be permanently cured, it can be effectively managed with consistent treatment to the point where symptoms remain minimal and hair loss is prevented.
Can stress cause seborrheic dermatitis?
Stress does not directly cause seborrheic dermatitis but is a well-documented trigger for flares. Elevated cortisol from chronic stress increases sebum production and suppresses immune regulation, both of which promote Malassezia overgrowth and the inflammatory response characteristic of SD. Managing stress through regular exercise, adequate sleep, and relaxation techniques can measurably reduce flare frequency.
Will hair grow back after treating seborrheic dermatitis?
Yes, in approximately 85-90% of cases. Once scalp inflammation is resolved, follicles that were pushed into the telogen (resting) phase by inflammation will re-enter the anagen (growth) phase. Visible regrowth typically begins within 3-4 months and continues improving for up to 12 months. If no regrowth is seen after 6 months of successful SD treatment, an overlapping condition like androgenetic alopecia should be investigated.
Is seborrheic dermatitis contagious?
No. Seborrheic dermatitis is not contagious. While the Malassezia yeast involved is naturally present on over 90% of human scalps, the condition results from an individual’s abnormal immune and inflammatory response to the yeast, not from person-to-person transmission.
Can I use coconut oil for seborrheic dermatitis?
Coconut oil has documented antifungal properties due to its lauric acid content. However, results are mixed for seborrheic dermatitis specifically. Coconut oil is comedogenic (pore-clogging) and may worsen seborrheic dermatitis in patients with oily scalps by providing additional lipids for Malassezia to metabolise. If you wish to try it, do a 2-week patch test on a small area before full application. It is not a substitute for medicated treatment.
What foods make seborrheic dermatitis worse?
While no definitive diet-SD link has been established through large clinical trials, observational evidence and dermatological consensus suggest that high-glycaemic foods (sugar, refined carbohydrates), excessive dairy, and alcohol may worsen flares by increasing sebum production and systemic inflammation. Anti-inflammatory diets rich in omega-3 fatty acids (fish, flaxseed), zinc (pumpkin seeds, legumes), and B-vitamins may help reduce severity.
When should I see a doctor for seborrheic dermatitis and hair loss?
See a qualified dermatologist if over-the-counter medicated shampoos do not improve your condition within 4 weeks, if hair loss continues despite scalp improvement, if you notice patchy bald spots, or if the condition spreads to your face or body. At Assure Clinic, our team of 60+ qualified doctors can differentiate between seborrheic dermatitis, psoriasis, alopecia areata, and androgenetic alopecia using trichoscopy, ensuring you receive the correct diagnosis and targeted treatment. Call +91 95861 22444 to book a consultation.
Conclusion
Seborrheic dermatitis is a chronic but highly treatable scalp condition. The hair loss it causes is, in the vast majority of cases, fully reversible with proper medical management. The key is accurate diagnosis, targeted antifungal treatment, and, when needed, adjunctive hair regeneration therapies.
If you have been battling scalp flaking, redness, and hair thinning, do not assume it is “just dandruff” or wait for it to resolve on its own. Early intervention prevents the transition from reversible inflammation-driven shedding to permanent follicular damage.
Take the next step:
- Call: +91 95861 22444
- WhatsApp: +91 95861 22444
- Assess your risk: Try the Baldness Calculator to understand your hair loss pattern
- Learn more: Explore hair fall reasons and hair fall control options
Assure Clinic’s 60+ qualified doctors across 13 locations in India and Dubai are ready to help you reclaim a healthy scalp and fuller hair.
Book a consultation to diagnose seborrheic dermatitis and start a how to stop hair fall plan tailored to you.